d-Transposition of the Great Arteries
What is it?
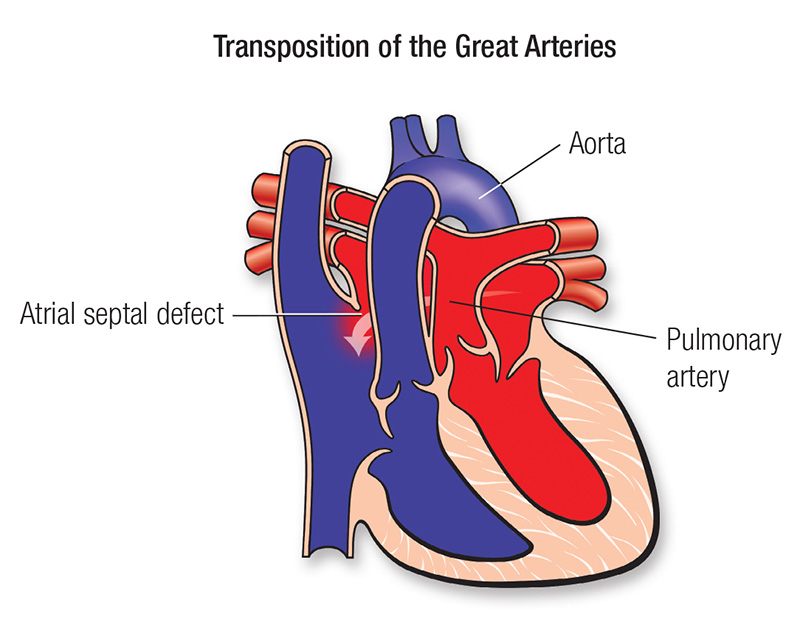
A heart in which the two main arteries carrying blood away from the heart are reversed.
A normal blood pattern carries blood in a cycle: body-heart-lungs-heart-body.
When a d-transposition occurs, the blood pathway is impaired because the two arteries are connecting to the wrong chambers in the heart.
This means that the blood flow cycle is stuck in either:
- body–heart –body (without being routed to the lungs for oxygen) or
- lungs–heart–lungs (without delivering oxygen to the body)
Without surgery, the only way to survive this condition temporarily is to have leakages that allow some oxygen-rich blood to cross into the oxygen-poor blood for delivery to the body. A hospital facility can also catheterize a patient until corrective surgery can be performed.
More information for parents of children with d-transposition
What about surgical treatment?
Patients with transposition of the great arteries require surgery early in life to survive. Many infants undergo a procedure in the catheterization laboratory to "buy time" and delay the surgery until they can handle it better. The procedure enlarges a naturally occurring connection between the right and left upper chambers (the atria). This lets the blood mix so some oxygen-rich and oxygen-poor blood can be pumped to the correct side.
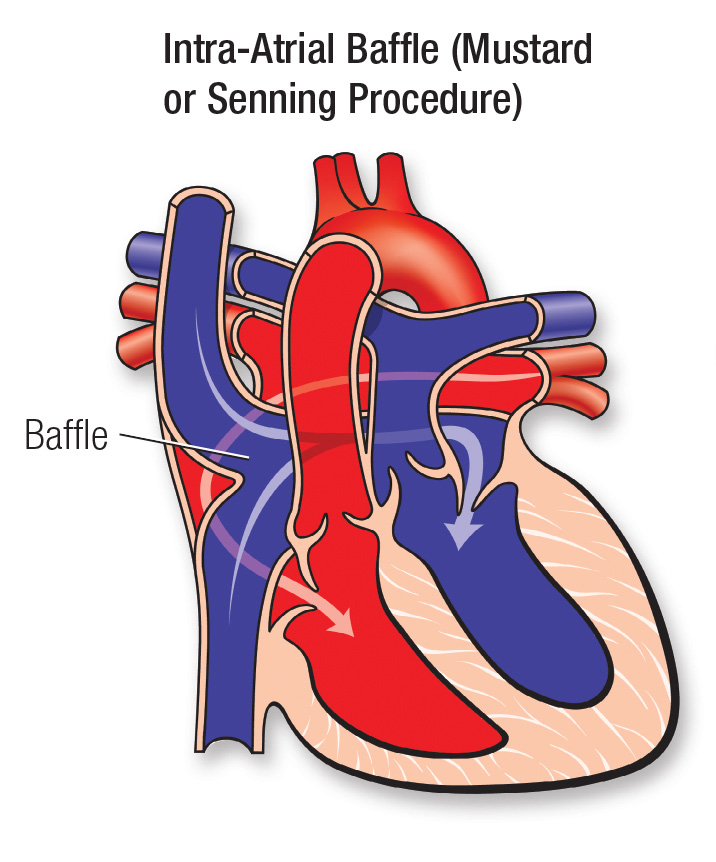
Two major types of surgery can correct the transposition. The first creates a tunnel (baffle) between the atria. This redirects the oxygen-rich blood to the right ventricle and aorta and the oxygen-poor blood to the left ventricle and the pulmonary artery. This operation is called an atrial switch. It's also called the Mustard or Senning procedure and is currently reserved for very rare cases.
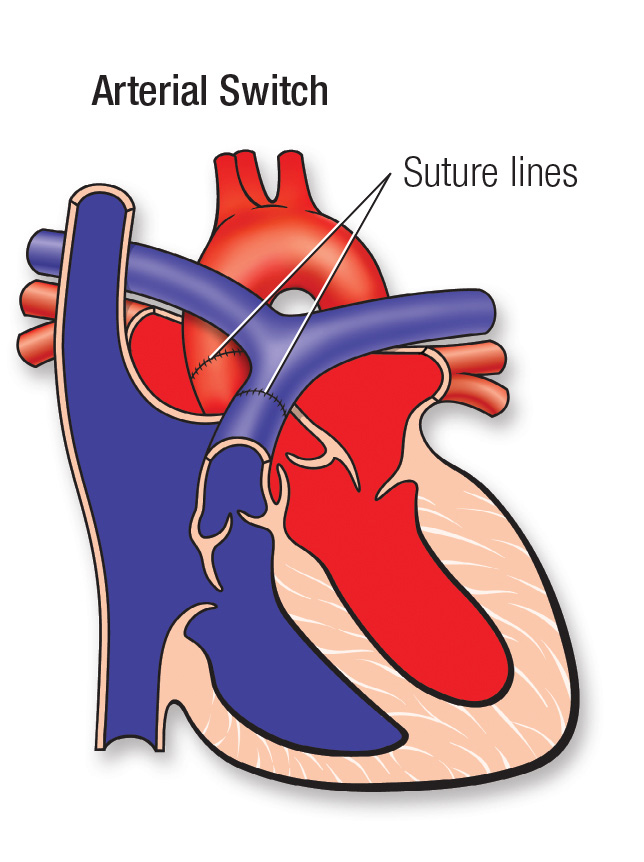
The second type is called the arterial switch operation. The aorta and pulmonary artery are switched back to their normal positions. The aorta is connected to the left ventricle, and the pulmonary artery is connected to the right ventricle. The coronary arteries, which carry the oxygen-rich blood that nourishes the heart muscle, also need to be reattached to the new aorta.
What type of problems might my child have?
Heart function problems
Patients who've had an atrial switch (e.g., Mustard or Senning operation) may have a serious decline in heart muscle or heart valve function. This is because the right ventricle is pumping blood to the entire body instead of just the lungs. Medications to help the heart pump better, control fluid accumulation (diuretics) and control blood pressure may help. Patients who've had the arterial switch operation don't seem to have as great a risk of heart muscle decline. They may have valve leakage or coronary artery problems, however.
Heart rhythm problems (Arrhythmias)
People with repaired transposition, especially those who've had the Mustard or Senning operation, are at risk of developing heart rhythm abnormalities (arrhythmias). These arrhythmias often arise in the heart's upper chambers. Your child's heart rate may be too slow or too fast. If the heart rate is too slow, an artificial pacemaker can speed it up. If your child's heart rate is too fast, medication can slow it down. At times, your child may need a cardiac catheterization to study and treat these rhythm disturbances.
Will my child need more surgery?
Some patients need more surgery to help their heart pump better, repair abnormal valves or control heart rhythm disturbances. Patients who've had the Mustard or Senning operation may need surgery to correct abnormalities of the tunnel in the atria, repair abnormal valves or control rhythm disturbances.
Patients who had the arterial switch operation may need more surgery to relieve narrowings in the aorta or pulmonary artery where the original surgery was done, or to fix leaky valves.
Will my child's activities be limited?
Most cardiologists recommend that patients limit their physical activities to their endurance. They don't recommend competitive sports for high school and college students. Your child's cardiologist will help determine the proper level of activity restriction.
What will my child need in the future?
Patients with transposition will require lifelong follow-up with a cardiologist trained to care for patients with congenital heart disease. Your child may need to take medications to improve how his or her heart works. The cardiologist will track your child with a variety of non-invasive tests. These include electrocardiograms, Holter monitors, exercise stress tests and echocardiograms.
What about preventing endocarditis?
Children who have transposition of the great arteries are at increased risk for endocarditis. Some children will need to take antibiotics before certain dental procedures. See the section on Endocarditis for more information.
Congenital Heart Defect ID sheet
More information for adults with d-transposition
What causes it?
The cause is unknown, but genetic factors may contribute to it. Pregnant mothers with uncontrolled diabetes are at higher risk of having children with transposition.
How does it affect the heart?
In this condition, the oxygen rich blood goes to the lungs and the oxygen poor blood goes to the body. All the parts are there, but the blood with the most oxygen (red blood) goes to the wrong place. The lack of oxygen can cause severe damage to the heart muscle in a short time.
How does it affect me?
Babies born with transposition are blue. If there are no connections between the right and left side of the heart to allow the oxygen poor and oxygen rich blood to mix, the baby can only survive for a short time (days). Some type of surgical treatment is needed to allow for survival throughout childhood and into adulthood. That's why virtually all adults with this condition have had surgery. The adult often has a number of medical problems related to the previous surgery as well as to problems that couldn't be repaired.
What can I expect from the transposition that was repaired in childhood?
As an infant you may have had a procedure in the catheterization laboratory to "buy time" and delay the surgery until you could handle it better. The procedure enlarged the naturally occurring connection between the right and left upper chambers (the atria). This lets the blood mix so some oxygen-rich and oxygen-poor blood can be pumped to the correct side. This communication is repaired when further surgery is done.
Two major types of surgery can correct the transposition. The first, developed in the late 1950s, creates a tunnel (a baffle) between the atria. This redirects the oxygen-rich blood to the right ventricle and aorta and the oxygen-poor blood to the left ventricle and the pulmonary artery. This operation is called an atrial or venous switch. It's also called the Mustard procedure or the Senning procedure.
The second type is called the arterial switch operation. It wasn't done routinely until the mid-1980s. The aorta and pulmonary arteries are switched back to their normal positions. The aorta is connected to the left ventricle, and the pulmonary artery is connected to the right ventricle. The coronary arteries, which carry the oxygen-rich blood that nourishes the heart muscle, also need to be re-attached to the new aorta. The arterial switch is now the preferred operation.
Can further repair be done in adulthood?
In rare cases, an adult patient who had an atrial switch operation may be a candidate for a takedown of their original operation and conversion to an arterial switch operation. This is more complicated than it sounds because this operation changes the main pumping chamber of the heart from the right to the left ventricle. Special additional procedures need to be done to prepare the left ventricle for this operation and they add considerable risk. This operation is only being done at a limited number of centers and usually only in adolescents or young adults.
Problems you may have
Patients who have undergone the Senning or Mustard procedures may have problems as they enter their twenties and thirties. The surgery in the atrium leaves areas of scar that can result in abnormal heart rhythms. Since the right ventricle remains the heart's main pumping chamber, it can become weakened, resulting in signs and symptoms of congestive heart failure. About half of patients will develop blockage in the baffles that were created to reroute the blood flow.
Theoretically, the arterial switch will have a much lower complication rate in adulthood than the atrial switch. This has been true in the early follow-up but the operation hasn't been done for a long enough time to know what problems may occur later in life. Patients may have valve leakage or coronary artery problems.
Ongoing Care
What will I need in the future?
All patients with repaired transposition require routine care by a specialist in the care of adults with congenital heart disease. Routine evaluation may include EKG, echocardiogram, Holter monitor and stress testing. Your cardiologist may recommend other testing such as MRI or heart catheterization. If you have a pacemaker, you will need more frequent visits. You should also consult a cardiologist with expertise in caring for adults with congenital heart disease if you're undergoing any type of non-heart surgery or invasive procedure.
Medical Treatment and Follow-up
Medications to help the heart pump better, control fluid accumulation (diuretics) and control blood pressure may help with congestive heart failure symptoms. Some patients with very slow heart rates may require a pacemaker. Those with rapid heart rates will require medication to control them or a special cardiac catheterization (electrophysiology study) to study and treat these rhythm disturbances may be needed. See the Arrhythmias section for more information. Obstructions in the baffles can often be treated with stents to enlarge the obstructed regions.
Activity Restrictions
Many patients won't need to limit their activity, especially those who have undergone the arterial switch. It's generally recommended that patients with atrial switch operations avoid activities such as weight lifting that cause a rise in blood pressure. However, if your heart doesn't pump normally or you have heart rhythm issues, you may need to limit your activity to your endurance. Your cardiologist will help determine if you need to limit your activity. See the Physical Activity section for more information.
Preventing Endocarditis
People who have transposition of the great arteries and had atrial switch operations require endocarditis prophylaxis. Most patients who underwent simple arterial switch procedures won't need prophylaxis. Your cardiologist will be able to determine if you need to keep taking routine antibiotics before certain dental work. See the section on Endocarditis for more information.
Pregnancy
Women with repaired transposition may have successful pregnancies. The risk from pregnancy to the mother increases if heart failure or arrhythmias exist. It's important to consult with a cardiologist experienced in caring for patients with congenital heart defects before pregnancy to find out the health risks. See the section on Pregnancy for more information. It is also for women with transposition to be seen in centers with high risk obstetrical services and adult congenital heart disease expertise.
Will I need more surgery?
Patients who have had the Mustard or Senning operation may need catheterization techniques or surgery to correct abnormalities of the tunnel in the atria, repair abnormal valves or control rhythm disturbances. Slow as well as fast heart rhythms are common so many patients with these operations need pacemakers eventually.
Patients who had the arterial switch operation infrequently may need more surgery to relieve narrowing in the aorta or pulmonary artery where the original surgery was done, or to fix leaky valves.







